|
|
|||
| What is the optimal neoadjuvant endocrine therapy and when should it be used? | |||
|
|
||||||||||
|
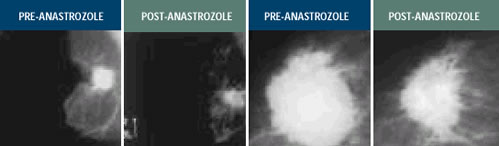
Chemotherapy is the most frequent form of neoadjuvant systemic therapy in the United States; while in Europe, endocrine therapy has been utilized extensively in women with ER-positive cancers. Numerous phase 2 and 3 clinical trials have demonstrated that the antitumor effect of endocrine therapy in these patients is comparable to what has been observed with chemotherapy, although the time to response is somewhat longer. Tamoxifen and ovarian ablation/suppression were initially utilized, and more recently, studies of third-generation aromatase inhibitors have demonstrated significant antitumor activity. NEOADJUVANT ENDOCRINE THERAPY RESEARCH BACKGROUND We began studying neoadjuvant systemic therapy about 15 years ago. What’s clear is that you can obtain a very good idea of what’s happening within the tumors by looking at biological markers rather than just clinical endpoints. To determine if we can predict early on whether a patient is going to receive benefit from therapy, we take biopsies 10 to 14 days after treatment and examine effects on proliferation, cell death and a variety of genetic markers. This becomes a potential method to individualize treatment. We found the median time to reduce tumor volume is shorter with chemotherapy than with endocrine therapy. However, the same order of response is seen with endocrine therapy — you just have to wait a bit longer. —J Michael Dixon, MD, FRCS The studies in ER-positive, postmenopausal women showed a very high degree of antitumor activity in patients treated with aromatase inhibitors. In one trial, anastrozole showed dramatic tumor reductions — 70% or 80% of the patients showed objective shrinkage of their disease, and close to two-thirds of the women became candidates for breast preservation after approximately four months of therapy with anastrozole. —Aman Buzdar, MD EORTC STUDY 10963 The preoperative EORTC trial evaluates one injection of fulvestrant after the diagnosis of breast cancer but before surgery. The idea is for the fulvestrant injection to cover the operative period as a potent antiestrogen that will lower estrogen receptor levels. We want to test the hypothesis of Bernie Fisher and others that adverse events related to metastases occur during the perioperative period. Hopefully, we can alter that with fulvestrant. The aim is to enroll more than 3,000 women into this study. —J Michael Dixon, MD, FRCS PROPOSED NEOADJUVANT TRIAL We are looking for a trial to replace ATAC and are considering evaluating conventionally timed versus perioperative endocrine therapy. Fulvestrant lends itself to that because of its rapid effects on the tumor in situ, and you can measure surrogate markers. We would like to take the best arm of ATAC and compare it with fulvestrant in a factorial way — looking at drug against drug and timing against timing. Hopefully, we’ll have a pilot protocol ready to go next year. This type of trial — where you’re looking at the tumor intact — can be a gold mine in the search for the valuable surrogate markers of response. —Michael Baum, ChM, FRCS
Cheung KL et al. Preoperative endocrine therapy for breast cancer. Endocrine-Related Cancer 1999;7(3):131-141. Full Text Dixon JM et al. The effects of neoadjuvant anastrozole (Arimidex) on tumor volume in postmenopausal women with breast cancer: A randomized, double-blind, single-center study. Clin Cancer Res 2000;6(6):2229-35. Abstract Hoff PM et al. Combined modality treatment of locally advanced breast carcinoma in elderly patients or patients with severe comorbid conditions using tamoxifen as the primary therapy. Cancer 2000;88(9):2054-60. Abstract Milla-Santos A et al. Anastrozole (A) as neoadjuvant (NEO) therapy for hormone-dependent locally advanced breast cancer (LABC) in postmenopausal (PM) patients (pts). Breast Cancer Res Treat 2001; Abstract 302. Bundred N et al. ICI 182,780 (Faslodex) an estrogen receptor downregulator reduces cell turnover index more effectively than tamoxifen. Proc ASCO 2001;Abstract 1660. Abstract Robertson JFR et al. The pharmacokinetics of single dose FaslodexTM (ICI 182,780) in postmenopausal primary breast cancer — Relationship with estrogen receptor (ER) down regulation. Proc ASCO 2000;Abstract 362.
|