|
||||||||
| Tracks 1-19 | ||||||||||||||||||||||||||||||||||||||||
|
Select Excerpts from the Interview
Tracks 2-3
![]() DR LOVE: Can you review the design and key findings from NSABP-B-27?
DR LOVE: Can you review the design and key findings from NSABP-B-27?
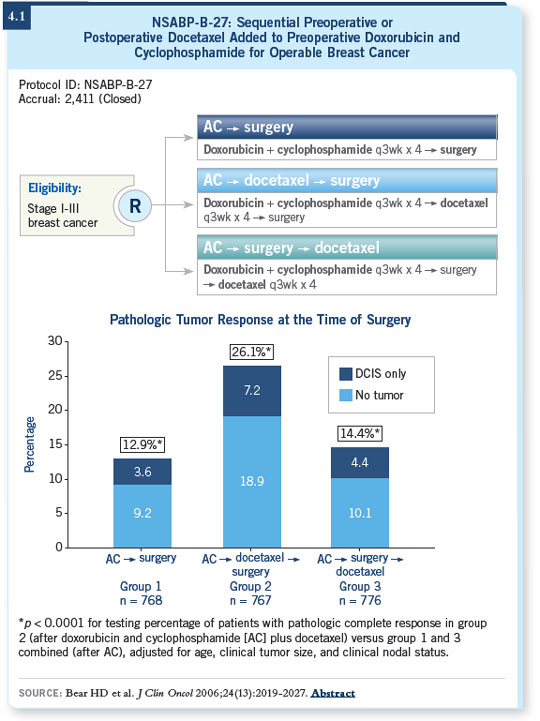
![]() DR BEAR: NSABP-B-27 was the successor to NSABP-B-18, which was a randomized trial of four cycles of preoperative versus postoperative AC (Wolmark 2001). In NSABP-B-27 the objective was to determine whether adding four cycles of either preoperative or postoperative docetaxel to four cycles of preoperative AC would improve patient outcomes (Bear 2006; [4.1]).
DR BEAR: NSABP-B-27 was the successor to NSABP-B-18, which was a randomized trial of four cycles of preoperative versus postoperative AC (Wolmark 2001). In NSABP-B-27 the objective was to determine whether adding four cycles of either preoperative or postoperative docetaxel to four cycles of preoperative AC would improve patient outcomes (Bear 2006; [4.1]).
We also wanted to correlate the addition of preoperative docetaxel with improvements in response, particularly pathologic response in the breast, which we had shown in NSABP-B-18 to be the most powerful predictor of patient outcomes (Wolmark 2001). We found that preoperative docetaxel almost doubled the pathologic complete response rate in the breast (Bear 2003; [4.1]).
It is surprising that we did not see a statistically significant improvement in either disease-free or overall survival with the addition of preoperative or postoperative docetaxel (Bear 2006). I believe there are a number of potential reasons. Some have attributed it to the concurrent use of tamoxifen, but I am not sure that is entirely correct. Concurrent tamoxifen may have somewhat degraded the chemotherapy’s effects, but we saw no interaction between hormone receptor status and the effect of docetaxel (Bear 2006).
![]() DR LOVE: The issue of responsiveness to chemotherapy based on ER status is a hot topic. Where do you think the NSABP-B-27 data fit in?
DR LOVE: The issue of responsiveness to chemotherapy based on ER status is a hot topic. Where do you think the NSABP-B-27 data fit in?
![]() DR BEAR: The NSABP-B-27 data are a little problematic because we don’t have the hormone receptor status on all patients. From those patients for whom we had the pretreatment hormone receptor status, our data were like the TAC trial. The patients with either ER-negative or ER-positive disease had a significantly higher pathologic complete response rate with docetaxel and AC than with AC alone (Bear 2003).
DR BEAR: The NSABP-B-27 data are a little problematic because we don’t have the hormone receptor status on all patients. From those patients for whom we had the pretreatment hormone receptor status, our data were like the TAC trial. The patients with either ER-negative or ER-positive disease had a significantly higher pathologic complete response rate with docetaxel and AC than with AC alone (Bear 2003).
In a subset analysis of NSABP-B-27, we also analyzed the benefit of docetaxel according to whether the patients responded clinically to AC. We found that patients who did not respond to AC did not benefit from docetaxel, indicating that those were probably patients with chemoresistant disease and that the addition of another chemotherapy drug probably didn’t help much (Bear 2006).
Among patients who had a clinical complete response to AC, we also did not see much benefit from docetaxel, indicating that those are probably patients with good-prognosis chemoresponsive disease. The group of patients who had a clinical partial response to AC was the most interesting. Those patients showed a significant improvement in disease-free survival with the addition of preoperative docetaxel (Bear 2006).
One might ask why those patients who had a clinical partial response to AC didn’t benefit from postoperative docetaxel (Bear 2006). I suspect it’s because of the delay in the administration of the second chemotherapy regimen. The delay between completing AC and starting docetaxel may have negated the benefit by allowing the regrowth of metastatic clones.
Track 5
![]() DR LOVE: What is a reasonable approach to neoadjuvant chemotherapy outside of a study?
DR LOVE: What is a reasonable approach to neoadjuvant chemotherapy outside of a study?
![]() DR BEAR: For a patient who has been chosen for neoadjuvant treatment because of a large tumor, I would use an anthracycline-with-taxane-based regimen. Some people use TAC in this situation, although we have no data with neoadjuvant TAC. I would choose a sequential regimen, such as AC followed by docetaxel, FAC followed by weekly paclitaxel or weekly paclitaxel followed by FAC.
DR BEAR: For a patient who has been chosen for neoadjuvant treatment because of a large tumor, I would use an anthracycline-with-taxane-based regimen. Some people use TAC in this situation, although we have no data with neoadjuvant TAC. I would choose a sequential regimen, such as AC followed by docetaxel, FAC followed by weekly paclitaxel or weekly paclitaxel followed by FAC.
I believe waiting to administer the additional treatment postoperatively offers no advantage and potentially carries a disadvantage. For most of the patients who really need neoadjuvant chemotherapy, I believe there is nothing wrong with committing them to an aggressive treatment course, as we would a patient with node-positive disease.
Track 7
![]() DR LOVE: Can you talk about the new NSABP-B-40 neoadjuvant trial?
DR LOVE: Can you talk about the new NSABP-B-40 neoadjuvant trial?
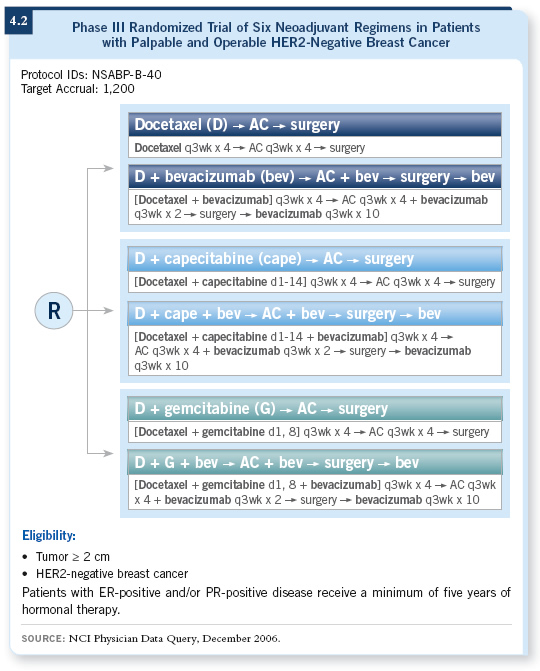
![]() DR BEAR: NSABP-B-40 (4.2) has evolved over a long period of time. We were hampered by not knowing the results of NSABP-B-27, but we wound up using AC followed by docetaxel as the control regimen.
DR BEAR: NSABP-B-40 (4.2) has evolved over a long period of time. We were hampered by not knowing the results of NSABP-B-27, but we wound up using AC followed by docetaxel as the control regimen.
From the very beginning we wanted to evaluate the effect of adding a biologic response modifier. We observed many agents over the period of years this trial has been developed, and each one did not pan out to have the activity that we thought indicated it would be useful. Bevacizumab has come along recently as a promising drug not only in the metastatic setting (Miller 2005) but also in the locally advanced neoadjuvant setting.
We are now poised to take a number of actions with NSABP-B-40 (4.2). One is to examine docetaxel combined with capecitabine or gemcitabine as a potential way to increase the response rate and improve patient outcomes. Another is to add bevacizumab to chemotherapy for half of the patients in the three different chemotherapy groups.
We will administer docetaxel or docetaxel doublets first, which is different from our previous design and is mainly being done to take advantage of the documented synergy between a taxane and bevacizumab. It will also allow us to stop bevacizumab two months or so before surgery so we don’t run into surgical complications as a result of angiogenesis inhibition.
NSABP-B-40 will involve docetaxel, docetaxel with capecitabine, or docetaxel with gemcitabine administered every three weeks for four cycles followed by AC for four cycles. Bevacizumab will be used during the first six cycles of chemotherapy, and then those patients who are randomly assigned to preoperative bevacizumab will also receive 10 cycles of postoperative bevacizumab.
One of the exciting things about this study is the attempt to further understand the mechanism of action of bevacizumab. We have evidence that macroscopic tumor shrinkage may be synergistic between bevacizumab and chemotherapy, and the NCI showed nicely that cancer cells express VEGF receptor and the phosphorylation of that receptor is dramatically downregulated in patients who respond to bevacizumab, so there may be a significant effect on the tumor cells directly and on the tumor’s blood supply.
Track 13
![]() DR LOVE: Another area of research in the NSABP that I wanted to ask you about was the Oncotype DX assay.
DR LOVE: Another area of research in the NSABP that I wanted to ask you about was the Oncotype DX assay.
![]() DR BEAR: The Oncotype DX assay was developed through a joint effort of Genomic Health and NSABP. It required a number of steps, one of which was to figure out how to measure gene expression in paraffin-fixed tissue.
DR BEAR: The Oncotype DX assay was developed through a joint effort of Genomic Health and NSABP. It required a number of steps, one of which was to figure out how to measure gene expression in paraffin-fixed tissue.
Once that was worked out, the next step was to determine whether we could find a limited number of genes that when combined could be used as a prognostic indicator for patient outcomes (Paik 2004).
To do that, we went back to NSABP-B-14, a trial in which patients were randomly allocated to receive either tamoxifen alone or no treatment. All the patients in NSABP-B-14 had ER-positive, node-negative disease. Then the assay was validated in another group of patients who were treated with tamoxifen. It has also been validated in a separate group of patients not in the trial.
In practical terms, for a patient with a hormone-responsive, small to moderate-size tumor faced with the decision about taking hormonal therapy alone or in combination with chemotherapy, we have a way to measure their residual risk and the likelihood they will derive a benefit from chemotherapy (Paik 2004, 2006).
In our working group, we are talking about applying this kind of profiling to patients with node-positive disease. It’s not clear that just because a patient has node-positive disease she will necessarily have a bad outcome or benefit from chemotherapy. We’re talking about our next generation of what we used to call “node-positive trials.”
We are approaching the time when we will consider trials for patients with high-risk disease. Those trials would include patients with negative nodes and a high recurrence score, and they may exclude patients with positive nodes and a low recurrence score. I believe Soon Paik is in the process of evaluating some of our trials for patients with node-positive disease to determine whether we can in fact identify those with node-positive disease who have a low risk.
![]() DR LOVE: Gary Lyman, with others, examined the economics of the
Oncotype DX and found it to be cost effective. For patients at low risk, you can avoid the cost of chemotherapy and, conversely, for patients at high risk who choose chemotherapy, you can significantly reduce the risk of recurrence and the subsequent cost of treatment.
DR LOVE: Gary Lyman, with others, examined the economics of the
Oncotype DX and found it to be cost effective. For patients at low risk, you can avoid the cost of chemotherapy and, conversely, for patients at high risk who choose chemotherapy, you can significantly reduce the risk of recurrence and the subsequent cost of treatment.
![]() DR BEAR: Chemotherapy can cost $20,000 to $30,000, whereas the assay is $3,500. It requires a careful analysis of how many patients forego chemotherapy
as a result of the assay and the money you save to offset the cost of performing the tests in patients who do receive chemotherapy. From a noneconomist’s perspective, that is, someone who is not an expert in cost effectiveness, it does seem logical that it would be cost effective, but it takes a more careful analysis to prove it.
DR BEAR: Chemotherapy can cost $20,000 to $30,000, whereas the assay is $3,500. It requires a careful analysis of how many patients forego chemotherapy
as a result of the assay and the money you save to offset the cost of performing the tests in patients who do receive chemotherapy. From a noneconomist’s perspective, that is, someone who is not an expert in cost effectiveness, it does seem logical that it would be cost effective, but it takes a more careful analysis to prove it.
Tracks 15-16
![]() DR LOVE: What has been your usual approach in terms of adjuvant hormonal therapy for postmenopausal patients?
DR LOVE: What has been your usual approach in terms of adjuvant hormonal therapy for postmenopausal patients?
![]() DR BEAR: By and large, postmenopausal patients who do not already have osteoporosis are receiving aromatase inhibitors up front. The ATAC results are difficult to dispute. With patients who have been on tamoxifen for a year, I haven’t jumped to switching them to an aromatase inhibitor.
DR BEAR: By and large, postmenopausal patients who do not already have osteoporosis are receiving aromatase inhibitors up front. The ATAC results are difficult to dispute. With patients who have been on tamoxifen for a year, I haven’t jumped to switching them to an aromatase inhibitor.
I will probably follow the paradigm of some of the other trials and leave them on tamoxifen for two or three years, then I’ll switch them over. I believe they will obtain some bone-density benefit by staying on tamoxifen for a while and start out at a better baseline when we switch them over to an aromatase inhibitor.
NSABP-B-42 will address the question of duration of hormonal therapy. It will examine the group of patients who have received five years of either a combination of tamoxifen and an aromatase inhibitor or an aromatase inhibitor alone. The trial will determine whether those patients should receive an aromatase inhibitor for another five years. It’s a five- versus 10-year question, reminiscent of the NSABP-B-14 rerandomization.
![]() DR LOVE: What is your opinion about the safety and tolerability of the aromatase inhibitors compared to tamoxifen?
DR LOVE: What is your opinion about the safety and tolerability of the aromatase inhibitors compared to tamoxifen?
![]() DR BEAR: The aromatase inhibitors bring some advantages compared to tamoxifen in terms of the risk of uterine cancer, which is not an issue if a woman has had a hysterectomy. The concerns about osteopenia and osteoporosis are probably the biggest downsides to the aromatase inhibitors.
Monitoring or treatment with bisphosphonates is required to limit the morbidity. The aromatase inhibitors have other side effects. I have had a number of patients who cannot tolerate them because of the muscle aches, et cetera. We can always go back to tamoxifen, if they are willing. The aromatase
inhibitors may cause fewer or less severe hot flashes, although they still cause them.
DR BEAR: The aromatase inhibitors bring some advantages compared to tamoxifen in terms of the risk of uterine cancer, which is not an issue if a woman has had a hysterectomy. The concerns about osteopenia and osteoporosis are probably the biggest downsides to the aromatase inhibitors.
Monitoring or treatment with bisphosphonates is required to limit the morbidity. The aromatase inhibitors have other side effects. I have had a number of patients who cannot tolerate them because of the muscle aches, et cetera. We can always go back to tamoxifen, if they are willing. The aromatase
inhibitors may cause fewer or less severe hot flashes, although they still cause them.