|
||||||||
| Tracks 1-14 | ||||||||||||||||||||||||||||||
|
Select Excerpts from the Interview
Track 2
![]() DR LOVE: Could you describe the SWOG neoadjuvant trial presented at ASCO 2006?
DR LOVE: Could you describe the SWOG neoadjuvant trial presented at ASCO 2006?
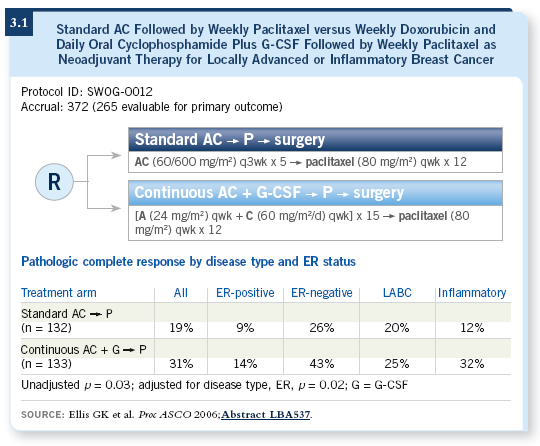
![]() DR LIVINGSTON: SWOG-S0012 was designed for women with locally advanced and inflammatory breast cancer and randomized patients to AC followed by weekly paclitaxel (T) versus weekly doxorubicin and daily oral cyclophosphamide with G-CSF followed by T. The eligibility criteria were fairly standard. Most typically, patients with locally advanced breast cancer had a tumor measuring five centimeters or greater, but they could also be enrolled if they had Stage III disease by other criteria. For patients with inflammatory disease, the diagnosis was made on a clinical basis with pathologic confirmation.
Standard treatment for these patients in the community has been anthracycline-based neoadjuvant chemotherapy.
DR LIVINGSTON: SWOG-S0012 was designed for women with locally advanced and inflammatory breast cancer and randomized patients to AC followed by weekly paclitaxel (T) versus weekly doxorubicin and daily oral cyclophosphamide with G-CSF followed by T. The eligibility criteria were fairly standard. Most typically, patients with locally advanced breast cancer had a tumor measuring five centimeters or greater, but they could also be enrolled if they had Stage III disease by other criteria. For patients with inflammatory disease, the diagnosis was made on a clinical basis with pathologic confirmation.
Standard treatment for these patients in the community has been anthracycline-based neoadjuvant chemotherapy.
Our primary endpoint in the study was pathologic complete response, and the only variable studied was the method of administration of AC because the paclitaxel was given in the same way to all patients.
The MD Anderson group and others have shown that pathologic complete response (pCR) is a very good predictor of long-term outcome for these patients. It is defined as the disappearance of all evidence of invasive disease under the microscope when the pathologist examines the specimen after completion of chemotherapy.
At ASCO 2006, my colleague Dr Georgiana Ellis presented the data for the first 265 out of 398 patients entered (Ellis 2006). The pCR was 31 percent for the continuous arm — the experimental arm — versus 19 percent for the standard arm (3.1), which was statistically significant.
As you might expect, the toxicity data indicated less myelosuppression for the experimental arm, and that’s because those patients received prophylactic G-CSF. In terms of other toxicities, more stomatitis and hand-foot syndrome occurred with the experimental regimen. More nausea, vomiting and myelo-suppression occurred on the standard arm. Both regimens were well tolerated, and more than 95 percent of the patients entered on the study were able to go to surgery.
We will be conducting another analysis, but it seems likely that the continuous administration of AC is better than the every three-week administration. That furnishes, of course, a strong rationale for trying to finish SWOG-S0221, the current adjuvant trial for patients with node-positive disease, in which the randomization basically involves every two-week or dose-dense therapy.
Track 4
![]() DR LOVE: In SWOG-S0012, was there any correlation between the ER-status or HER2-status and outcome?
DR LOVE: In SWOG-S0012, was there any correlation between the ER-status or HER2-status and outcome?
![]() DR LIVINGSTON: Patients were eligible regardless of their ER and HER2 status. This trial preceded the release of information about the value of adjuvant trastuzumab, so none of the patients received trastuzumab.
DR LIVINGSTON: Patients were eligible regardless of their ER and HER2 status. This trial preceded the release of information about the value of adjuvant trastuzumab, so none of the patients received trastuzumab.
When we did subgroup analyses, we saw that the pathologic complete response rate for patients with hormone receptor-negative disease — ER-negative and PR-negative — was strikingly higher for those patients in the experimental versus the standard arm, 43 versus 26 percent (3.1). Although a trend favors the experimental therapy for patients with hormone receptor-positive disease, the pathologic complete response rate in the experimental arm is only 14 percent versus nine percent in the standard arm.
These results are in line with what most other investigators have reported: The benefit in terms of the pathologic complete response rate with anthracycline-based chemotherapy, with or without a taxane, appears to be much more striking among the patients with hormone receptor-negative disease (3.1).
When we examined data from the patients with HER2-positive disease, which was 28 percent of those entered on the trial, interestingly, we saw no evidence of an advantage for the continuous arm versus the standard arm. Both arms had a pathologic complete response rate of approximately 25 percent.The other group of patients who appeared to show a striking benefit were those with inflammatory breast cancer, which was a third of the patients entered on the study.
Track 6
![]() DR LOVE: What is your opinion regarding the clinical use of nanoparticle albumin-bound (nab) paclitaxel? Do you feel we need trials to demonstrate that it’s equivalent to or better than paclitaxel, given the advantage of the infusion time and the lack of premedication in all clinical situations?
DR LOVE: What is your opinion regarding the clinical use of nanoparticle albumin-bound (nab) paclitaxel? Do you feel we need trials to demonstrate that it’s equivalent to or better than paclitaxel, given the advantage of the infusion time and the lack of premedication in all clinical situations?
![]() DR LIVINGSTON: We have a fair amount of data, both from preclinical systems and from clinical trials, to suggest that the drug is superior to paclitaxel,
independent of its ability to prevent allergic reactions.
DR LIVINGSTON: We have a fair amount of data, both from preclinical systems and from clinical trials, to suggest that the drug is superior to paclitaxel,
independent of its ability to prevent allergic reactions.
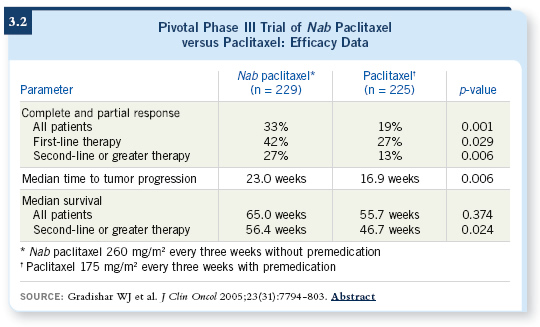
A reputable randomized study published in the Journal of Clinical Oncology compared nab paclitaxel to paclitaxel on an every three-week schedule for women with metastatic breast cancer (Gradishar 2005; [3.2]). That study shows a magnitude of improvement in terms of response rate and time to progression, which is fairly similar to the magnitude of difference that was demonstrated in ECOG-E2100 between paclitaxel alone and paclitaxel with bevacizumab (Miller 2005).
However, the paclitaxel with bevacizumab trial was accepted with great enthusiasm — legitimately — and presented in a fairly frenzied special oral session at ASCO, while the trial involving nab paclitaxel versus paclitaxel was basically disregarded.
In my own practice, I’m prescribing patients paclitaxel because of the cost differential. If cost were not an issue, I would stop administering paclitaxel today and substitute it with nab paclitaxel.
Track 7
![]() DR LOVE: Can you discuss more about what we know in terms of clinical research with neoadjuvant bevacizumab and comment on the study reported by Sandy Swain’s group at the NCI (Wedam 2006)?
DR LOVE: Can you discuss more about what we know in terms of clinical research with neoadjuvant bevacizumab and comment on the study reported by Sandy Swain’s group at the NCI (Wedam 2006)?
![]() DR LIVINGSTON: The interesting part of that study, of course, has to do with the run-in phase, during which the patients receive bevacizumab alone. Investigators performed serial tumor sampling and were able to demonstrate down-modulation of appropriate targets for angiogenesis. It was a nice in vivo demonstration that the drug does have an effect on the expected target, the VEGF receptor.
DR LIVINGSTON: The interesting part of that study, of course, has to do with the run-in phase, during which the patients receive bevacizumab alone. Investigators performed serial tumor sampling and were able to demonstrate down-modulation of appropriate targets for angiogenesis. It was a nice in vivo demonstration that the drug does have an effect on the expected target, the VEGF receptor.
The other observation from the Swain trial, which she has perhaps downplayed a little bit, was the difficulty with postoperative complications in patients who had received bevacizumab up until a few weeks prior to surgery. Certainly that provided a take-home message, together with the colorectal experience, to the rest of us that this drug does stick around for several weeks.
Track 11
![]() DR LOVE: What are your thoughts about TOPO II and response to systemic therapy? Do you think it’s ready for prime time?
DR LOVE: What are your thoughts about TOPO II and response to systemic therapy? Do you think it’s ready for prime time?
![]() DR LIVINGSTON: I believe we need more data, but the data will be coming very soon. A completed Southwest Oncology Group trial (9313) is in press in the Journal of Clinical Oncology.
DR LIVINGSTON: I believe we need more data, but the data will be coming very soon. A completed Southwest Oncology Group trial (9313) is in press in the Journal of Clinical Oncology.
Importantly, all the patients in that study received AC. In that study, Larry Norton’s single-agent sequenced A ![]() C was compared to concurrent AC, and no difference appeared between the two, which is rather “ho-hum.”
C was compared to concurrent AC, and no difference appeared between the two, which is rather “ho-hum.”
However, we have tumor material from all those patients who received an anthracycline and have long-term follow-up available. I suspect that data will be presented soon on the correlation between the presence or absence of TOPO II amplification and benefit from an anthracycline-based regimen.
We should see no difference between the two arms, but we would expect to see a tremendously better result in patients with TOPO II amplification who are receiving an anthracycline than in patients without TOPO II amplification.
![]() DR LOVE: What about that issue for the patient with HER2-positive disease?
DR LOVE: What about that issue for the patient with HER2-positive disease?
![]() DR LIVINGSTON: Certainly the data from BCIRG 006 that Dennis Slamon presented in December of last year at San Antonio suggest that an anthracycline-based regimen is superior for women with HER2-positive disease if they have TOPO II amplification and is not superior if TOPO II is not amplified (Press 2005; Slamon 2005). Thirty-five percent of the patients have TOPO II amplification.
DR LIVINGSTON: Certainly the data from BCIRG 006 that Dennis Slamon presented in December of last year at San Antonio suggest that an anthracycline-based regimen is superior for women with HER2-positive disease if they have TOPO II amplification and is not superior if TOPO II is not amplified (Press 2005; Slamon 2005). Thirty-five percent of the patients have TOPO II amplification.
Remember that although those curves looked impressive, the follow-up and number of events are not yet sufficient for the p-value to be statistically significant. We need more information.
Track 12
![]() DR LOVE: What chemotherapy would you consider for patients with triple-negative, node-positive disease?
DR LOVE: What chemotherapy would you consider for patients with triple-negative, node-positive disease?
![]() DR LIVINGSTON: Patients with triple-negative, node-positive disease are perhaps the single greatest therapeutic challenge right now. In terms of management off study, I am offering those patients aggressive treatment. I’m offering them our metronomic version of AC with growth factor support followed by weekly paclitaxel. Having said that, I don’t believe this is enough.
DR LIVINGSTON: Patients with triple-negative, node-positive disease are perhaps the single greatest therapeutic challenge right now. In terms of management off study, I am offering those patients aggressive treatment. I’m offering them our metronomic version of AC with growth factor support followed by weekly paclitaxel. Having said that, I don’t believe this is enough.
This is a patient population that cries out for well-designed therapeutic trials. We know, for example, that those patients with triple-negative disease appear to have a fairly high incidence of overexpression of the EGF receptor by immunohistochemistry.
Does that mean that they might benefit from the administration of targeted therapy, such as either a monoclonal antibody or a small molecule directed at the EGF receptor? We simply don’t know the answer.
The second issue that is hinted at, especially by work out of the University of Chicago group, is that even women with the “sporadic” triple-negative cancers, setting aside the BCRA1 mutations, appear to have a fairly high incidence of down-regulation of BRCA1 function, meaning that their cancer cells are relatively sensitive to agents that produce DNA injury and require DNA repair. Remember, BRCA1 is a DNA repair-causing gene.
From data that were presented in San Antonio, in cell lines derived from such patients, the platinums appear to be quite active (Nanda 2005). It may be that triple-negative patients with high-risk disease should receive a platinum. It may be that those patients should receive an EGF receptor-targeted drug. But would I give them either one of these outside of a study right now? No, we will have to conduct studies to find out.
Tracks 13-14
![]() DR LOVE: In general, how would you approach the choice of chemotherapy
DR LOVE: In general, how would you approach the choice of chemotherapy
and the question of bevacizumab for a patient with moderately symptomatic, triple-negative metastatic disease?
![]() DR LIVINGSTON: We do not have hard evidence that one chemotherapy regimen is better than another chemotherapy regimen for the patient you just described.
DR LIVINGSTON: We do not have hard evidence that one chemotherapy regimen is better than another chemotherapy regimen for the patient you just described.
I believe most of us would be inclined to use anthracycline-based therapy if the patient hadn’t received it previously or if it had been more than a year since completion of her adjuvant treatment.
Many of us would be inclined to use a combination rather than a single agent, and I’m one of those because these patients have particularly aggressive disease and tend to experience short times to progression. The delay in time to progression that one sees with combinations may be important for patients with this type of disease.
At both my earlier institutional affiliation in Seattle and in the Southwest Oncology Group, we have been exploring antitubulin combinations, investigating combinations of vinorelbine and a taxane, either docetaxel or paclitaxel.
Most recently, I’ve been involved in a trial with nab paclitaxel and vinorelbine. Those combinations are active. What I can honestly tell you is they’re probably not more active than somebody else’s choice of docetaxel and capecitabine or gemcitabine-based therapy.
![]() DR LOVE: What about bevacizumab?
DR LOVE: What about bevacizumab?
![]() DR LIVINGSTON: The only patient right now, outside of a study, for whom I would probably urge the use of bevacizumab is this individual you’ve just described, because we do have evidence that the taxanes are as active, if not more active, than any other drugs. We do have evidence that weekly paclitaxel,
which is the best way to administer the drug, is potentiated by the use of bevacizumab.
DR LIVINGSTON: The only patient right now, outside of a study, for whom I would probably urge the use of bevacizumab is this individual you’ve just described, because we do have evidence that the taxanes are as active, if not more active, than any other drugs. We do have evidence that weekly paclitaxel,
which is the best way to administer the drug, is potentiated by the use of bevacizumab.
And we do have, in the triple-negatives, a group of patients for whom, right now, no targeted therapy is available, except bevacizumab, that we can justify on the basis of a randomized trial. So if I were seeing such a patient in the clinic today, I would talk to her about a taxane-based treatment program, in all likelihood, and I would recommend that she also receive bevacizumab.